

The role of impaired capillary blood flow in ME
As long ago as the 1980s, Dr Les Simpson in New Zealand found that the red blood cells of patients with CFIDS were deformed and when deformed, they cannot get through the capillary bed, causing pain.
This article was specially commissioned for Invest in ME Research's Journal of IiME that appeared in 2008 - and can be seen here in pdf form and here in flip page format.
Leslie Owen Simpson currently lived in Dunedin, New Zealand, but also lived in 6 countries and from 1991 travelled and lectured extensively.
Hegraduated from the University of Otago, majoring in botany and zoology and later worked in the field of tissue transplantation.
He became a WHO lecturer in medical biology at the Central Medical School, Suva, Fiji, with a brief to establish a medical biology department and train technical staff.After a spell in teaching he was appointed research officer in the Pathology Department, Otago Medical School, studying the pathobiology of the first animal model of lupus erythematosus, the NZ Black Mouse.
After a postdoctorate in experimental pathology he worked as a senior research officer.Although retired in 1985 he continued to work full time in unpaid appointments as honorary research fellow, first in the Pathology Department and then in the Department of General Practice. In 1999 he set up Red Blood Cell Research Limited and continued his research on red blood cells and privately funded much of the research.
He had 125 letters or articles published in medical journals as well as numerous other articles in journals and textbooks.
INTRODUCTION
There is no doubt that one of the major problems facing those who suffer from myalgic encephalomyelitis (ME) is the persisting disagreements about the name of the disorder. To a great extent this was exemplified by a group in Florida who decided to change CFS to ME. For that reason alone it is important to recognise Ramsay’s concept of ME so that those with the problem can be identified and separated from other illnesses such as chronic fatigue syndrome (CFS) and post-viral fatigue syndrome (PVFS). Until this happens, ME people will continue to be disadvantaged.
In the preface to the second edition of his book,
“Myalgic encephalomyelitis and postviral fatigue
states,” published in 1988, Dr.Ramsay wrote, “When on
the occasion of a recent ITV programme on the subject
of myalgic encephalomyelitis, an immunologist stated
that ‘ME and PVFS are regarded as synonyms’ I realised
that my objection to the latter term was fully justified
and that it was incumbent on me to show that such a
statement is blatantly untrue.” He stated also, “The
clinical identity of the myalgic encephalomyelitis
syndrome rests on three distinct features, namely:
1. a unique form of muscle fatigability whereby, after
even a minor degree of physical effort, three, four
or five days, or longer elapse before full muscle
power is restored;
2. variability and fluctuation of both symptoms and
physical findings in the course of a day:
3. an alarming tendency to become chronic.”
In the text, Ramsay discussed the multiplicity of symptoms in three groups. 1. Muscle phenomena. He noted, when discussing the time for the restoration of normal muscle power, “…it is important to stress the fact that cases of ME of mild or even moderate severity may have normal muscle power in a remission.” 2. Circulatory impairment. This was manifested as cold extremities and facial pallor. 3. Cerebral dysfunction was manifested in many ways including memory problems, difficulties with concentration and emotional lability. It seems rather surprising that Ramsay did not link the dysfunction of muscles and brain to the recognised problems of circulatory impairment. He stated however, “The chronic case can take two different forms. In the first there is a recurring cycle of remission and relapse. In three doctors who contracted the infection between 1955 and 1958, the alternation of remission and relapse continues. The second form is more tragic and no remission occurs.” It is clear that remissions play a large part in Ramsay’s concept of ME.
The introduction, by the Centers for Disease Control in the USA, in 1988, of the term chronic fatigue syndrome (CFS), almost immediately made life more complicated for ME sufferers, as the criteria for CFS were much more inclusive. Not only were ME patients gathered under the CFS umbrella, but also the results of Americans studying CFS tended to be adopted as being relevant to ME, and to a large extent Ramsay’s experience was ignored. In most countries, despite the opposition of small groups, ME people were diagnosed as having CFS, even though there were no accepted
pathophysiologies for either diagnosis. To a large extent this is the current situation. For example, a 2001 English publication titled “What is ME? What is CFS?” (1) discussed ME mainly in terms of the findings of American investigators, only a 1981 paper by Ramsay was quoted and no reference was made to either edition of his book. In 2007, The Nightingale Research Foundation published, “The Nightingale myalgic encephalomyelitis definition,” (2) even though in their 1992 book, Dr.Hyde had suggested that “encephalopathy” was a more appropriate term. Primary ME was defined as, “…an acute onset biphasic epidemic or endemic (sporadic) infectious disease process where there is always measurable and persistent diffuse vascular injury of the CNS in both the acute and chronic phases. Primary ME is associated with immune and other pathologies.” The concept of “…persistent diffuse vascular injury,” would rule out any involvement of Ramsay-style remissions. It is clear that the possible role for shapechanged red cells as recorded in my paper in the 1992 book, was rejected.
At a meeting of Canadian and American investigators who were interested in ME, a consensus was reached and released as the Canadian Consensus. In 2007, a review was published under the title, “Definitions and aetiology of myalgic encephalomyelitis: how the Canadian consensus clinical definition of myalgic encephalomyelitis works.”(3) It was noted, “To improve clinical observation, the Canadian definition and diagnostic protocol lays out several regions of pathophysiological dysfunction, as necessary components of the syndrome of myalgic encephalomyelitis, but the particular expression of symptoms within each region is contingent between individuals and their particular pattern is left open to be decided by clinical observation of the individual and later diagnostic classification.” This 59 word sentence is typical of the writing, but the enclosed message is far from clear.
It was noted also, that, “The possible aetiology of myalgic encephalomyelitis is under scientific observation. This is done by experiment and by controlled observation. Many observers are following various lines of investigation and observation as to the aetiology of myalgic encephalomyelitis, which we are following with interest.” This statement seems not to recognise that ME has been studied for 50 years. The crucial factor is whether or not like is being compared with like. Given the degrees of difference in the various definitions, there seems to be a grave danger that apples are being compared to oranges.
In general, two features of the paper stand out. No mention was made of Ramsay’s work or of remissions and there was no indication that blood flow was a problem. Therefore it seems that because of the conflicting views of experts and a general lack of agreement concerning the aetiology and pathophysiology of ME, a small section of the community will continue to suffer a reduced quality of life while experiencing a variety of symptoms, which, if they are lucky may disappear for variable periods of time during remissions.
WHO IS AT RISK OF DEVELOPING ME?
In any group of people who suffer from the same viral infection, most return to full health in less than 14 days, while a small proportion become chronically unwell. This implies that those who continue to be unwell (?ME people) are different from the normal population in some feature.
About the time I became involved with ME in 1983, I was developing an interest in the measurement of blood viscosity and blood filterability. Initially I studied blood samples from the blood donor panel, but through the good offices of Prof.J.C.Murdoch, who had a clinical interest in ME, I obtained blood samples from 21 female and 11 male patients with ME. Control samples were obtained from age and gender matched blood donors. Blood viscosity was measured at four shear rates and blood was filtered through polycarbonate filters with 5 micron pores at four levels of negative pressure. The results were published in 1986 (4) and showed that although there were differences in the results from blood viscometry of ME people and controls, they did not reach statistical significance. In contrast, at the lowest filtration pressure, the values for ME females were significantly different from controls, (an indication of stiffened red cells) but the differences in the male values did not reach significance. An examination of the data revealed that some ME values were near normal and would have influenced the results. The implications of the results were that ME people could be at risk of blood flow problems in the microcirculation because of the effects of poorly deformable red cells. It should be noted that for the assessment of filterability, EDTA-anticoagulated blood was used and filtration took place within half an hour of the sample being drawn. Subsequent developments from the simple technique included the washing of the red cells in saline, but such treatment greatly changed blood filterability. Our report concluded, “ … advances in our understanding of the aetiology of the disorder will come from investigations in the acute phase, and blood rheology may be of value in identifying those who are acutely affected.” Although non-ME subjects may have poorly filterable blood for 12 to 14 days after an infection, ME blood remains poorly filterable as long as they are symptomatic.
So ME people respond to agents which change the internal environment, by stimulating change in red cell shape and making them less deformable, probably because of a persisting, but unidentified factor in the blood. As will be discussed later, that factor has the capacity to switch off, resulting in a remission. Until the factor has been identified, it seems inappropriate to consider cure, as an endpoint and my objective in treatment is simply to improve the quality of life of sufferers.
To a large extent it seems that clinicians take red cells for granted, ignoring the fact that the loss of the nucleus as the cell leaves the bone marrow, renders it incapable of independent existence, and at the mercy of its environment. There are many published reports which record the different ways in which red cells respond to change in their environment, both in vivo and in vitro, with the change in shape associated with reduced deformability. The significance of the reduction in deformability is that the average diameter of capillaries lies between 3.5 and 5 microns, whereas the diameter of a red cell is between 7.5 and 8 microns. Therefore, in order to traverse a capillary bed, red cells must be able to deform and any reduction in red cell deformability will increase the resistance to flow in the microcirculation.
A 1970 editorial (5) titled, “The importance of
erythrocyte deformability,” concluded that,
“ …the remarkable deformability of normal mature
erythrocytes appears to depend on at least three
factors: (1) maintenance of the biconcave shape
which in turn depends on a high ratio of surface area to
cell volume; (2) normal internal fluidity of the cell which
in turn depends primarily on the properties of normal
haemoglobin; and finally (3) intrinsic membrane
deformability which is significantly affected by the
relationship between intracellular ATP, calcium and
magnesium and may be affected by pH and oxygen
tension in local regions of the microcirculation.”
Therefore it can be expected that any change in the cell environment which alters any of those three factors will lead to a reduction in cell deformability. Although viral infections, which will alter the internal environment, are considered to be key factors in the aetiology of ME, other infections, inoculations, vaccinations, severe emotional upsets, herbicidal sprays and heavy physical activity have been reported as causal factors in ME. All those factors will alter the red cell environment. However, it needs to be emphasised that although everyone exposed to such changes will show shapechanged red cells, only a small proportion will go on to develop the symptoms of ME.
So those who are at risk of developing ME have some physiological difference which leads to a reduced ability to restore red cell shapes to normal. The action of the unknown factor or factors involved may persist for 15 to 20 years or longer.
WHO GETS ME?
As the problems of poorly deformable red cells in traversing a capillary bed will be greatest in small capillaries, it is proposed that a key factor in determining who gets ME is the anatomical feature of smaller than usual capillaries. The random distribution of clusters of small capillaries provides a basis for understanding the idiosyncratic nature of the symptoms of ME. This implies that some cases may exhibit only a few regions which become symptomatic, whereas other cases may have symptoms in many regions of the body. While the presence of smaller than usual capillaries may have little functional effects when red cells exhibit normal deformability, their presence will become obvious after exposure to an agent which alters the internal environment and stimulates change in the shape populations of red cells. Furthermore, during remissions, when red cell shape populations return to normal, normal functional status indicates normal rates of capillary blood flow.
Because a requirement for normal tissue function is a normal rate of capillary blood flow which delivers sufficient oxygen and nutrient substrates to sustain normal function and to remove metabolic wastes, it is clear that when shape-changed, poorly deformable red cells are in the circulation, capillary blood flow will not be normal. The severity of the consequences of impaired capillary blood flow will be determined by the tissue involved. Muscles, the central nervous system and secreting glands are particularly sensitive to oxygen deprivation which may lead to body wide dysfunction. It is not surprising that in ME most symptoms relate to those tissues.
Therefore it is proposed that those people who develop
the chronic condition we call ME, share the common
anatomical feature of having smaller than usual
capillaries, the distribution of which will be marked by
the development of symptoms when some agent
induces change in red cell shape which makes them
poorly deformable. Because many other chronic
disorders exhibit changes in the shape populations of
red cells, the presence of such cells is not diagnostic for
ME. A 1992 paper (6) noted that,
“ Subjects with the characteristic (of smaller than usual capillaries)
would always be at risk of developing red cell shaperelated
impairment of capillary blood flow.”
Thus, those who will get ME are the small proportion of the population who by chance have smaller than usual capillaries. The severity of the symptoms which develop in the presence of poorly deformable red cells will reflect the extent to which small capillaries are present in the microcirculation. Limited observations have left me with the impression that black and brownskinned races have a lower incidence of small capillaries.
BLOOD FILTERABILITY AND RED CELL SHAPE
The findings of reduced blood filterability stimulated the thought that some change in the surface features of red cells might be involved (in the terms of Weed’s concept). To explore this possibility, a technique used for the rapid examination of theatre specimens by electron microscopy was adapted to study red cell morphology. The key factor was that the blood samples (3 to 5 drops of venous blood) were fixed immediately by being added to 5ml of 2.5% glutaraldehyde in 0.1M cacodylate buffer at pH 7.4. After fixation for overnight, at least, the cells were dehydrated in ascending concentrations of ethanol to absolute, then passed through three changes of pure, dry acetone. A drop of the acetone-suspended red cells was placed on a glass cover slip fixed to an aluminium stub with double sided adhesive tape. After air-drying, the cells were gold-coated in a sputter coater, then photographed under standard conditions in a scanning electron microscope. The cells in the resulting micrographs were classified into six different shape classes and the proportions expressed as percentages of the total number of cells counted. The first series of blood samples assessed in this way came from healthy blood donors, and from the first sample it was clear that the current teaching that all red cells were biconcave discocytes was not sustainable.
In 1989 I was able to report that the red cells in immediately fixed blood samples from healthy animals and humans could be classified into six different shape classes.(7) Later in the year I reported that blood samples from patients with acute ME showed increased proportions of cup forms (stomatocytes), a form which is known to be poorly deformable. (8) At a meeting in India in 1992, I discussed the red cell shape changes which had been found in six chronic disorders. (9)
Studies of the relevant literature, while preparing those reports, revealed that there had been earlier reports concerning changes in the shape populations of red cells. From 1974-78, there had been several reports concerning red cell shape in patients with muscular dystrophy. However, only one study (10) used immediately fixed blood samples, and the results were different from those studies which had manipulated the blood cells prior to fixation. The authors (10) noted that they were unable to prevent unfixed red cells from changing shape, even in their native plasma in a refrigerator. This is the expected response of red cells to a changing environment. In 1977, it was reported that patients with Huntington’s Disease had increased proportions of stomatocytes (cup forms). (11) Because increased proportions of stomatocytes would have an adverse effect on capillary blood flow, it is of interest that a 1985 study reported impairment of cerebral blood flow which was shown to correlate with cognitive impairment of patients with Huntington’s Disease.(12) Even though it was very likely that stomatocytes were responsible for the impaired cerebral blood flow, no reference was made to the 1977 study. In general there was no clinical interest in changed shape populations of red cells, and such reports provoked little continuing interest.
However, Mukherjee et al (13) were stimulated by our 1986 study of poorly filterable blood, to embark on a study of red cell morphology in ME people. They reported the presence of small numbers of grossly abnormal red cells. But the cells examined had been washed and centrifuged prior to fixation, and it is very likely that the abnormal cells were a result of the preparation technique. In the 13,000-odd immediately fixed blood samples relating to a number of chronic conditions in eight countries, which I have assessed, I have never seen a cell with the features of that described by Mukherjee et al.
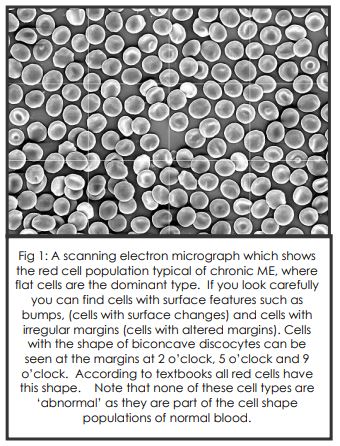
At the Cambridge Symposium on ME in 1990, I reported that blood samples from another 99 patients with acute ME showed similar values for increased cup forms to those of the previously reported 102 cases (14). It was noted also that there were small numbers of cases which presented with increased proportions of flat cells or cells with altered margins. In hindsight, it now seems likely that those changes were the beginning of a trend to chronic ME, as by 1992 only about 5% of cases were presenting with the cup forms of acute ME, and increased flat cells was the most common feature of chronic ME. It should be noted that the title of the paper I submitted made no mention of chronic fatigue syndrome, and this was added to the title by the editors, without discussion.
Thus, the information relating to reduced blood filterability is reinforced and possibly explained by the changed red cell morphology seen by scanning electron microscopy, so impaired capillary blood flow can be expected. What is important is that change in the cell shape populations is not a benign event. Remember, for example, that Weed (5) had noted that the deformability of red cells depended upon, “…maintenance of the biconcave shape.” Possibly of greater physiological importance were the findings of Vandergriff and Olson (15) that red cell shape was a determinant of the rate of uptake and release of oxygen. For example, crenated cells (cells with altered margins) were found to have a 45% reduction in the uptake of oxygen and a 23% reduction in release rate.
TIREDNESS, MUSCLE DYSFUNCTION AND CAPILLARY BLOOD FLOW
It is particularly unfortunate that the term ‘fatigue’ is
used so frequently in the ME literature. Both Funk and
Wagnall and the Oxford Concise dictionary define
fatigue as the consequence of long-continued exertion,
but ME people do not have to run up stairs to feel tired.
The authors of a 1921 study of industrial fatigue noted
that they could not measure or define ‘fatigue’ and it
was recommended that, “The term fatigue should be
absolutely banished from precise scientific discussion.”
(16) Sir John Ellis noted in a paper titled “Malaise and
fatigue,” (17) that patients seldom used such terms.
Instead, “They complain of being tired and not feeling
well…they say they are knackered, bushed, beat,
washed out, drained or utterly exhausted…. They add
that it started gradually some time ago, and then say
their tiredness is inexplicable.” Although the use of the
term ‘fatigue’ may invite controversy, muscle fatigue is
an accepted physiological condition. In accordance
with the idea that poorly deformable red cells would
impair capillary blood flow sufficiently for muscle
function to be interrupted by an inadequate oxygen
delivery rate, this concept was tested in ME people and
in healthy subjects. A healthy young woman acted as a
guinea pig and it was found that the repeated pulling of
a trigger until trigger finger fatigue, led to a three-fold
increase in cells with altered margins in the 35 seconds
taken to induce muscle fatigue. (18) Unexpectedly, in
applying for approval for a study involving ME people,
the Ethics Committee ruled that ME was an unknown
entity, but approval was obtained by substituting
“subjects with chronic tiredness,” for ME. The study took
place at a weekend residential meeting of members of
ME support groups where 69 ME volunteers took part.
(19) After a 5-drop blood sample had been taken, the
trigger of a model revolver was pulled repeatedly until
the onset of trigger finger fatigue. A second blood
sample was obtained and the
number of trigger pulls and the elapsed time were
recorded. Five minutes later the procedure was
repeated. Subsequently the procedure was repeated
in 72 healthy controls who were police officers, firemen,
army personnel, nurses and teachers. In general, the
results showed that at baseline, ME people had
different red cell shape populations from controls and
they had fewer trigger pulls with greater changes in
their post-trigger pulling blood samples. It was
concluded that, “The association of increased
nondiscocytes and impaired muscle function could
indicate a cause and effect relationship. This would be
in agreement with the physiological concept of fatigue
as a consequence of inadequate oxygen delivery.”
So it is relevant that in his textbook of human physiology, (20) Griffiths noted that muscle fatigue probably was due to oxygen deficiency and the effects of localised accumulations of metabolites including lactic acid, “…when the metabolites were not removed because of impaired capillary blood flow.” Wiles et al (21) considered that energy generation would fail if there was an enzymatic block in the glycogenolytic pathway or if there was a failure of oxidative metabolism. They considered the limiting features of energy generation to be blood flow and oxygen delivery.
While much has been written about ‘Tired patients,’
and ‘Tiredness,’ a 1960 paper by Ffrench (22) is of
special interest. Ffrench considered that, “Tiredness is
a symptom rather than a clinical condition,” and that,
“Tiredness is a ‘whole’ symptom. It is felt throughout
the patient’s body and is not confined to regions,
anatomic structures or specific physiological functions,
but rather it emanates from the natural whole of the
human body and mind.” His study involved 1170
patients, of whom 105 complained of tiredness. After
discussing the possible contributions of a number of a
number of factors, Ffrench concluded, “There is no
doubt that oxygen lack is the first cause of tissue cell
exhaustion, which is manifested early by clinical
tiredness.”
BRAIN DYSFUNCTION AND CAPILLARY BLOOD FLOW
It is postulated that the effects of shape-changed, poorly deformable red cells will impair capillary blood flow on a wide basis, with the most severe effects relating to regions small capillaries in tissues which are sensitive to oxygen deprivation.
Because tiredness is a major problem for those who suffe from multiple sclerosis, (MS) at the conclusion of our 1986 study on ME, we investigated the filterability and other aspects of blood samples from members of the local Multiple Sclerosis Society. As with ME, the rate of blood filterability was much less than that of healthy controls and there were changes in red cell morphology. A possibly relevant implication of these changes is that in 1983, Swank et al (23) had shown by xenon washout that in MS subjects, “…there occurred a progressive, generalised decrease in cerebral blood flow and in red cell delivery with age, which was significantly greater than observed in normal subjects. The rate of decrease in cerebral blood flow and red cell delivery correlated directly with the rate of progress of the disease.
Studies using single photon computed tomography (SPET or SPECT) have shown in other conditions with shape-changed red cells, that there can be significant reductions in regional cerebral blood flow. The relevance of this is that on March 30 1994, Dr.D.C.Costa presented his findings from a SPET study of ME patients at the annual general meeting of the British Nuclear Medicine Society. He reported that ME/CFS patients, “… had a generalised reduction in brain perfusion, “ and that, “… brainstem blood flow was significantly lower than in patients with depression and that both patient groups had significantly lower brainstem blood flow than in healthy subjects.” Even though I had published three reports concerning the effects of nondiscocytic red cells in ME patients prior to 1994, Dr.Costa hypothesised that the reduced demand for oxygen in the brain related to an overactive immune system which resulted in an excessive production of cytokines.
Dr.Costa’s comparison of the cerebral blood flow of ME/CFS with depression draws attention to a significant literature concerning SPECT scans and depression. Perhaps the most informative was a study by Bench et al (24) which showed that a region of the brain with impaired blood flow during depression, showed normal blood flow rates when the depressive episode resolved.
Evidently the regions associated with reduced blood flow have diagnostic significance as shown in another study by Dr.Costa. Lucey, Costa et al (25) reported that in some psychiatric disorders, there were significant differences in regional cerebral blood flow, as defined by SPET. While whole brain blood flow correlated with anxiety, there were significant regional cerebral blood flow differences between patients with obsessive compulsive disorder and post-traumatic stress disorder and controls.
REMISSIONS – THE CORNER STONE OF RAMSAY’S CONCEPT OF ME.
Even though Ramsay had described remissions as a feature of ME, and gave examples of the remission/relapse cycle, remissions are unrecognised by American investigators and are little recognised in other countries. This situation could be a possible consequence of ME being considered as the result of a persistent infection or a persistent immunological abnormality, or the consequence of localised pathology, as such beliefs would be incompatible with the remissions which Ramsay recorded.
My first experience with a remission related to a young woman who delivered a blood sample about 9am one morning. She explained that she had been too unwell to have had a blood sample taken earlier. On checking the details on her blood test request form it was noted that she had checked the box ‘well with no symptoms.’ pointed out that if she was well when she had the blood drawn then it was likely that the results would be normal. About 4pm on the same day she returned with another blood sample. She had ‘crashed’ about 3.30pm, for no discernible reason, and gone to the laboratory for another sample. The request form was marked ‘severely unwell.’ When the samples had been assessed it was found that the morning sample was normal and the afternoon sample was grossly abnormal. What factor or factors switch off to restore red cell shape populations to normal with improved wellbeing, and switch on to become symptomatic with changed red cell shape populations, remain unknown. However, the observation is consistent with Ramsay’s comment that during remission muscle function returns to normal.
Those observations led to an attempt to gain some insight into the frequency of remissions and concomitant changes in ME people in New Zealand. A panel of 37 females and 11 males who had been diagnosed by a physician as having ME at least 2 years previously, gave informed consent to take part in a 40 week-long study. At commencement and at four-weekly intervals thereafter, the panel met to record their symptoms and level of wellbeing and to provide a 5-drop sample of venous blood for red cell shape analysis. A total of 519 blood samples (401 female, 118 male) were assessed.
While the majority of blood samples showed the increased flat cells of chronic ME, normal results occurred sporadically. At one extreme there were five women who were unwell and had abnormal blood tests in 11 of 11 blood samples. Because of the four-week space between samples it is not known if remissions had occurred in the interval or if the women were in the group noted by Ramsay, who did not have remissions. At the other extreme was a woman who was well, with normal blood tests in 6 of 11 samples. The most frequent result, for both sexes, was to have two remissions during the 40 weeks of the study. The findings led to the conclusion that remissions were not uncommon events.
Such findings are in accord with the idea that ME is a dysfunctional state arising from inadequate rates of delivery of oxygen and nutrient substrates, rather than a condition associated with tissue pathology. That viewpoint is consistent also, with the improved wellbeing of patients who respond to agents which improve red cel deformability and thus increase capillary blood flow.
TREATMENT OPTIONS
The major factors in the development of the dysfunctional state manifested as the symptoms of ME are the presence of randomly distributed clusters of small capillaries and the effects of shape-changed, poorly deformable red cells on the rate of capillary blood flow. As it is not possible to influence capillary size, treatment should be aimed at improving red cell deformability, as remissions show that the red cell changes are reversible.
1. Acute ME. As reported at the Cambridge Symposium, a chance event led to an investigation iiv into the possible benefits of injections of vitamin B12 as hydroxocobalamin. A female patient reported that her general practitioner had given her an injection of hydroxocobalamin (Neo-Cytamen) and within 24 hours she felt much better. A blood sample was taken and revealed that her level of cup forms was reduced greatly. However, another patient failed to benefit from a similar injection and there was no change in her cup form value. The improved status of the responder was maintained with injections at about 10 day intervals. Through the co-operation of general practitioners it was found that 15 of 29 cases of ME responded to injections of hydroxocobalamin with symptom relief and reduced cup forms. However, there is no explanation of the mode of action of the B12 or why it was ineffective in 50% of cases.
2. Chronic ME. Some understanding of how the red cell changes in chronic ME might be relieved is based upon two early studies which investigated the effects of prostaglandins on red blood cells. Kury et al (26) used a spin-labelling technique to assess factors in red cells which influenced cell deformability. They reported that prostaglandin E1 (PGE1) increased red cell deformability, while the pro-inflammatory prostaglandin E2 (PGE2) had the opposite effect. By means of a filtration technique based upon standardised paper filters, Rasmussen et al (27) showed that PGE1 improved the filtration rate, while PGE2 had the opposite effect. Those observations were consistent with the findings of Kury et al, but in addition it was reported that catecholamines also reduced the rate of filtration. That finding could help to explain why both emotional and physical stress are causal factors in the relapses of ME people.
Although cis-linoleic acid is the basic precursor for PGE1, it has to be elongated to gammalinolenic acid (GLA) in a reaction mediated by the enzyme delta-6- desaturase. However it is known that in a number of situations the enzyme becomes dysfunctional, impairing the synthesis of GLA. For that reason it has been found useful to use plant sources of GLA. The most effective source is oil of evening primrose although it is unclear why it is responsible for higher production of PGE1 than other plant oils, even if their GLA content is higher. Manku et al (28) have reported that 2 grams daily of oil of evening primrose had no effect on the blood levels of PGE1, while 4 grams daily of the oil caused a significant increase in the concentration of PGE1 in the blood. So at least 4 grams daily of oil of evening primrose is needed to be effective. It needs to be emphasised that for unexplained reasons, not all individuals respond to that dose of evening primrose oil.
The omega-3 fatty acids also have the ability to improve red cell deformability and may offer an alternative. The smallest omega-3 is the plant-derived alphalinolenic acid which requires a functional delta-6- desaturase to elongate it in the synthesis of eicosapentaenoic acid. Because of the potential problems of delta-6-desaturase it is preferable to take omega-3 in the form of fish oil which is rich in eicosapentaenoic and docosohexanoic acids. Having demonstrated previously, by the use of a spinlabelling technique, that the lipid bilayer of the membranes of diabetic red cells were very viscous, (29) Kamada et al (30) reported that sardine oil taken orally, increased the fluidity of the lipid bilayer and increased the cell deformability. Although some ME people have responded to fish oil, I have not been able to identify which patients will respond to what oil. A lack of funding has prevented investigations into the performance of the oils by double-blinded randomised studies. However, on the result sheets concerning red cell shape analyses, in addition to the results, and a copy of the micrograph there is a suggestion that the effects of the changed red cells might be reduced by a daily intake of 4 grams of oil of evening primrose or 6 grams of fish oil. It is noted also, that if no benefit is perceived by 6 weeks, then another treatment should be tried. A patient in Denmark failed to respond to evening primrose oil or fish oil, but responded to pentoxifylline.
About 1988 a medical detailer reported that a general practitioner in a country town (Oamaru) was using pentoxifylline (Trental) to treat his ME patients. But before I could arrange a meeting the doctor was killed in a freak accident at a car rally where he was acting as a marshal As many studies have shown that pentoxifylline improves red cell deformability and reduces blood viscosity, it has the properties to be helpful for ME people but no reports of its use in ME have been located.
Despite the lack of placebo-controlled studies, I have had many letters and emails from people who have responded to one of the oils, with a restoration of a nearnormal lifestyle. My responses to such messages emphasise the need to persist with the effective treatment, while at the same time recognising that they are not cured and are still at risk.
THE IMPORTANCE OF LIFESTYLE IN ME
Even though persistent tiredness is a daily problem, it has to be accepted that long-term bed rest will have an adverse effect on muscle function. For that reason the daily programme should include provision for a period of low-intensity physical activity, such as walking 50 yards up the street and back again. Each week the distance walked should be increased, maybe in concert with an increase in speed. An interesting observation relating to a daughter with fibromyalgia was that when she was immersed up to her chin in a warm physiotherapy pool, the buoyancy provided by the water allowed her to do arm and leg exercises that she could not do on dry land.
ME people should not get involved in arguments and they should walk away when they see stressful situations developing. Both arguments and stress may raise the blood levels of altered cells sufficiently to cause a relapse
Give careful consideration to the nature of your diet. High levels of fat and cholesterol increase the stiffness of red cells. Try and increase your dietary intake of green vegetables and of oily fish. If this is too expensive, have a tin of sardines in oil two or three times a week.
Because low temperatures have an adverse influence on blood viscosity, it is important to dress warmly and if possible spend your time in a warm room.
THE ORIGINS OF THE DATA ON WHICH MY CONCEPTS REST
According to the entries in my daily diary, between January 1991 and December 2000, I spoke to 274 meetings in six countries. Although the great majority were ME groups, in the USA and Canada, I met CFS and CFIDS groups also. From about 1997, fibromyalgia groups were included.
Either during such visits or later, arrangements were made for an experienced venepuncturist to collect 5 drop blood samples which were mixed immediately with fixative When the samples had been evaluated, reports were prepared and submitted for publication. However, reports submitted to Australian, New Zealand and South African journals were rejected.
After giving an illustrated lecture to an ME audience in Victoria, British Columbia, I was approached by Dr.Abram Hoffer who introduced himself as the editor of the Journal of Orthomolecular Medicine. He invited me to submit a written version of the talk he had just heard. So in early 1997, a paper titled, “Myalgic encephalomyelitis (ME): a haemorheological disorder manifested as impaired capillary blood flow,” was published. (J Orthomol Med 1997; 12: 69-76). Later in that year I was able to publish the red cell shape analysis results of blood samples from 1558 female and 620 male members of ME organisations in four countries. (J Orthomol Med 1997; 12 221-6) The numbers involved in that report are so large that it would be strange if the data were not relevant.
In other reports I have summarised the information provided by 632 Americans with chronic disorders, and the red cell shape analysis results. In addition there is a report relating to the blood samples from 623 women with fibromyalgia, who resided in four countries. An intriguing aspect of that report is that the blood samples showed similar high values for flat cells to those of people with chronic ME. However, an analysis of the symptom lists showed that the first recorded symptom by the majority of ME people was tiredness, whereas in the fibromyalgia group the first symptom was pain.
CONCLUSIONS
What began as a study of various aspects of the blood in ME people finished up as a study of the red cell shape populations in a wide range of chronic disorders. In those disorders which have been studied by SPECT scans, the reported reductions in regional cerebral blood flow were consistent with the expected effects of shapechanged, poorly deformable red cells.
So ME is only one of many chronic disorders with changed red cells which will impair capillary blood flow. It would seem that ME is unique insofar as the factor or factors responsible for the changes in red cell shape, can switch off. During the resulting remission, red cell shape populations return to normal. Unfortunately, at this time, there is no diagnostic feature which can identify the group identified by Ramsay as having unremitting ME.
Even though many different factors may initiate the blood changes which are typical of ME, it needs to be emphasised that the baseline changes may be increased by secondary factors which alter the internal environment, such as emotional stress or physical overactivity or hormonal changes as in the pre-menstrual week. Such changes will precipitate relapses. In addition, the immune response to inoculations, vaccinations or other infections will worsen the severity of symptoms and the level of body dysfunction.
While the search for the primary problem continues, in order to improve the quality of life of sufferers, urgent attention is needed to define the actions of agents which can improve the deformability of red blood cells in order to provide an effective treatment. However, because of the official reluctance to investigate the pathophysiology of ME, sufferers may need to explore the potential benefits of those agents which will improve red cell deformability, on their own initiative.
REFERENCES
1. Marshall EP, Williams M, Hooper M. What is ME? What is CFS? Information for clinicians and lawyers. December 2001.
2. Anonymous. The Nightingale myalgic encephalomyelitis (M.E.) definition. The Nightingale Research Foundation, Ottawa, Canada. January 29, 2007.
3. Carruthers BM. Definitions and aetiology of myalgic encephalomyelitis: how the Canadian consensus clinical definition of myalgic encephalomyelitis works J Clin Path 2007;60:117-9.
4. Simpson LO, Shand BI, Olds RJ. Blood rheology and myalgic encephalomyelitis: a pilot study. Pathology 1986;18:190-2.
5. Weed RI. The importance of erythrocyte deformability. Am J Med 1970;49: 147-50.
6. Simpson LO. Chronic tiredness and idiopathic chronic fatigue – a connection ? N J Med 1992;89: 211-6.
7. Simpson LO. Blood from healthy animals and humans contains nondiscocytic erythrocytes. Br J Haematol 1989;73: 561-4.
8. Simpson LO. Nondiscocytic erythrocytes in myalgic encephalomyelitis. NZ Med J 1989;102: 106-7.
9. Simpson LO. Red cell shape in health and disease. In: Swamy NVC, Megha Singh (eds) Physiological Fluid Dynamics III. Narosa Publishing House, New Delhi, 1992, pp 230-5.
10. Miller SE, Roses AD, Appel SH. Scanning electron microscopy studies in muscular dystrophy. Arch Neurol 1976; 33: 172-4.
11. Markesbery WR, Butterfield DA. Scanning electron microscope studies of erythrocytes in Huntington’s Disease. Biochem Biophys Res Commun 1977; 78: 560-4.
12. Tanahashi N, Meyer JS, Ishikawa Y, et al. Cerebral blood flow and cognitive testing correlate in Huntington’s Disease. Arch Neurol 1985; 42: 1169-75.
13. Mukherjee TM, Smith K, Maros K. Abnormal red cell morphology in myalgic encephalomyelitis. (letter) Lancet 1987;ii: 328-9.
14. Simpson LO. The role of nondiscocytic erythrocytes in the pathogenesis of myalgic encephalomyelitis/chronic fatigue syndrome. In: Hyde BM, Goldstein J, Levine P (eds) The clinical and scientific basis of myalgic encephalomyelitis/chronic fatigue syndrome. The Nightingale Research Foundation, Ottawa, Canada, 1992, pp 597-605.
15. Vandergriff KD, Olson JS. Morphological and physiological factors affecting oxygen uptake and release by red blood cells. J Biol Chem 1984; 259:12619-27.
16. Muscio B. Is a fatigue test possible ? A report to the Industrial Fatigue Research Board. Br J Psychol 1921;12: 31-46.
17. Ellis J. Malaise and fatigue. Symptoms that depress a doctor and should not. Br J Hosp Med 1984;32: 312-4.
18. Simpson LO. Red cell shape. (letter) NZ Med J 1993;106: 531.
19. Simpson LO, Murdoch JC, Herbison GP. Red cell shape changes following trigger finger fatigue in subjects with chronic tiredness and healthy controls. NZ Med J 1993;106: 104-7.
20. Griffiths M. An introduction to human physiology. New York, NY, MacMillan Publishing Co., Inc.,1981, pp 73-4. 21. Wiles CM, Jones DA, Edwards RHT. Fatigue in human metabolic myopathy. Ciba Symposium 1981;82: 264- 82.
22. Ffrench G. The clinical significance of tiredness. Canad MAJ 1960;82: 665-71.
23. Swank RL, Roth JG, Woody DC Jr. Cerebral blood flow and red cell delivery in normal subjects and in multiple sclerosis. Neurol Res 1983;5: 37-59.
24. Bench CJ, Frackowiak RS, Dolan RJ. Changes in regional cerebral blood flow on recovery from depression. Psychol Med 1995;25: 247-61.
25. Lucey JV, Costa DC, Adshead G, et al. Brain blood flow in anxiety disorders. OCD, panic disorder with agoraphobia and post-traumatic stress disorder on 99 TchMPAO single photon emission tomography (SPET). Br J Psychiatry 1997;171: 346-50.
26. Kury PG, Ramwell PW, McConnell HM. The effect of prostaglandin E1 and E2 on the human erythrocyte a monitored by spin labels. Biochim Biophys Res Commun 1974;56: 478-83.
27. Rasmussen H, Lake W, Allen JE. The effect of catecholamines and prostaglandins on rat and human erythrocytes. Biochim Biophys Acta 1975;411 63-73.